Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
|
|
|
- Millicent Bryan
- 5 years ago
- Views:
Transcription


1 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
2
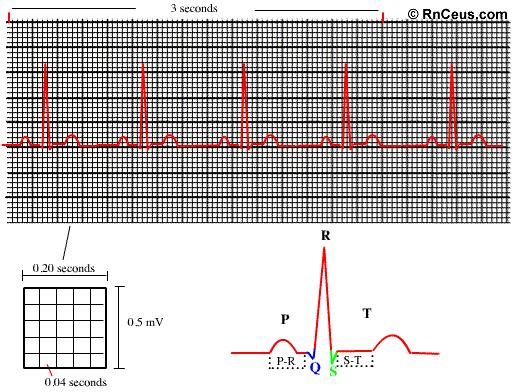
3 EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents 0.04 seconds. Each larger square is 5 mm in length and represents 0.2 seconds. Voltage is measured along the vertical axis
4 Voltage is measured along the vertical axis. 10 mm is equal to 1mV in voltage. The diagram below illustrates the configuration of EKG graph paper and where to measure the components of the EKG wave form
5
6 P wave Indicates atrial depolarization, or contraction of the atrium. Normal duration is not longer than 0.11 seconds (less than 3 small squares) Amplitude (height) is no more than 3 mm No notching or peaking
7 QRS complex Indicates ventricular depolarization, or contraction of the ventricles. Normally not longer than.10 seconds in duration Amplitude is not less than 5 mm in lead II or 9 mm in V3 and V4 R waves are deflected positively and the Q and S waves are negative
8 T wave Indicates ventricular repolarization Not more that 5 mm in amplitude in standard leads and 10 mm in precordial leads Rounded and asymmetrical
9 ST segment Indicates early ventricular repolarization Normally not depressed more than 0.5 mm May be elevated slightly in some leads (no more than 1 mm)
10 PR interval Indicates AV conduction time Duration time is 0.12 to 0.20 seconds QT interval Indicates repolarization time General rule: duration is less than half the preceding R-R interval
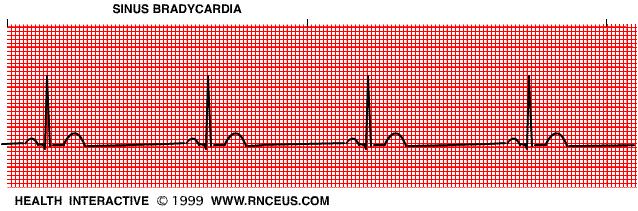
11 Sinus Bradycardia
12 Rate40-59 bpm P wavesinus QRSnormal ( ) ConductionP-R normal or slightly prolonged at slower rates Rhythmregular or slightly irregular
13 This rhythm is often seen as a normal variation in athletes, during sleep, or in response to a vagal maneuver. If the bradycardia becomes slower than the SA node pacemaker, a junctional rhythm may occur
14 Treatment includes: treat the underlying cause, atropine, isuprel, or artificial pacing if patient is hemodynamically compromised
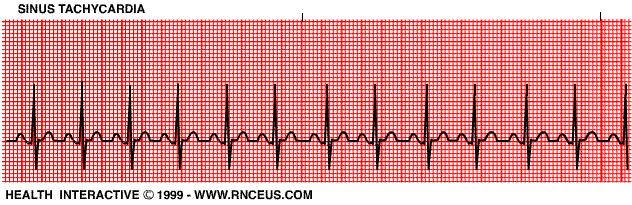
15 Sinus Tachycardia
16 Rate P wave QRS Conduction Rhythm /min sinus normal normal regular or slightly irregular
17 Underlying causes include The clinical significance of this dysrhythmia depends on the underlying cause. It may be normal. increased circulating catecholamines CHF hypoxia PE increased temperature stress response to pain
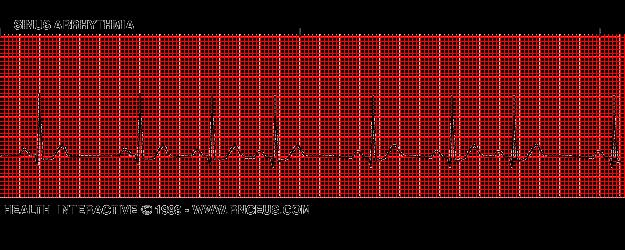
18 Sinus Arrhythmia
19 Rate P wave QRS Conduction Rhythm /bpm sinus normal normal regularly irregular
20 The rate usually increases with inspiration and decreases with expiration. This rhythm is most commonly seen with breathing due to fluctuations in parasympathetic vagal tone. During inspiration stretch receptors in the lungs stimulate the cardioinhibitory centers in the medulla via fibers in the vagus nerve.
21 The non respiratory form is present in diseased hearts and sometimes confused with sinus arrest (also known as "sinus pause"). Treatment is not usually required unless symptomatic bradycardia is present.

22 Wandering Atrial Pacemaker
23
24 This dysrhythmia may occur in normal hearts as a result of fluctuations in vagal tone. It may also be seen in patients with heart disease or COPD. Wandering atrial pacemaker may also be a precursor to multifocal atrial tachycardia. There is usually no treatment required

25 Premature Atrial Contractions
26
27 PAC's occur normally in a non diseased heart. However, if they occur frequently, they may lead to a more serious atrial dysrhythmias. They can also result from CHF, ischemia and COPD.

28 Sinus Arrest
29
30 This may occur in individuals with healthy hearts. It may also occur with increased vagal tone, myocarditis, MI, and digitalis toxicity. If the pause is prolonged, escape beats may occur. The treatment of this dysrhythmia depends on the underlying cause. If the cause is due to increased vagal tone and the patient is symptomatic, atropine may be indicated.
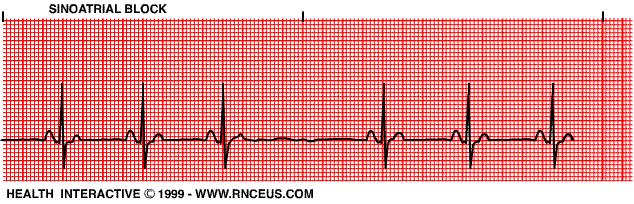
31 Sinoatrial Block
32
33 In a type I SA block, the P-P interval shortens until one P wave is dropped. *In a type II SA block, the P-P intervals are an exact multiple of the sinus cycle, and are regular before and after the dropped P wave. This usually occurs transiently and produces no symptoms. It may occur in healthy patients with increased vagal tone. It may also be found with CAD, inferior MI, and digitalis toxicity.

34 Multifocal Atrial Tachycardia
35
36 Multifocal atrial tachycardia (MAT) may resemble atrial fibrillation or flutter. It almost always occurs in seriously ill, elderly individuals. COPD is the most common underlying cause. Treatment depends upon the underlying cause

37 Paroxysmal Atrial Tachycardia
38
39 PAT may occur in the normal as well as diseased heart. It is a common complication of Wolfe-Parkinson- White syndrome. For more on WPW, click here. This rhythm is often transient and doesn't require treatment. However, it can be terminated with vagal maneuvers. Digoxin, antiarrhythmics, and cardioversion may be used

40 Atrial Flutter
41
42 Atrial flutter almost always occurs in diseased hearts. It frequently precipitates CHF. The treatment depends on the level of hemodynamic compromise. Cardioversion, vagal maneuvers and verapamil are used when prompt rate reduction is needed. Otherwise, digoxin and other antiarrhythmic drugs can be used.
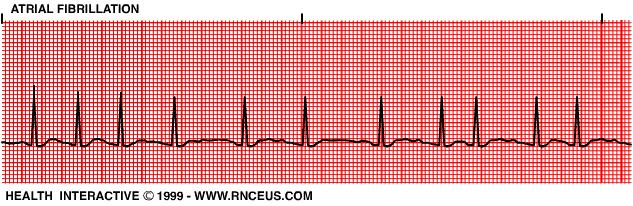
43 Atrial Fibrillation
44
45 Atrial fibrillation may occur paroxysmally, but it often becomes chronic. It is usually associated with COPD, CHF or other heart disease. Treatment includes: Digoxin to slow the AV conduction rate. Cardioversion may also be necessary to terminate this rhythm

46 Premature Junctional Contractions
47
48 PJCs may occur in both healthy and diseased hearts. If they are occasional, they are insignificant. If they are frequent, junctional tachycardia may result. Treatment is usually not required
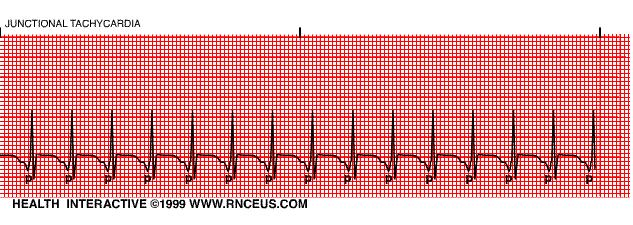
49 Junctional Tachycardia
50
51 The clinical significance of this rhythm depends upon the basic rhythm disturbance. If the ventricular rate is rapid, cardiac output may decrease. Treatment includes: finding and correcting the underlying cause, vagal maneuvers, verapamil, and cardioversion.

52 Junctional Escape Beats and Rhythm
53
54 The most common cause of this rhythm in healthy individuals is sinus bradycardia. It may also be seen in the presence of a high degree or complete AV block. If the ventricular rate is slow, hemodynamic compromise may occur. Treatment depends upon the underlying cause and the baseline dysrhythmias. Atropine or a pacemaker may be used to increase the ventricular rate
55 First Degree AV Block
56
57 This is the most common conduction disturbance. It occurs in both healthy and diseased hearts. First degree AV block can be due to: inferior MI, digitalis toxicity hyperkalemia increased vagal tone acute rheumatic fever myocarditis. Interventions include treating the underlying cause and observing for progression to a more advanced AV block.

58 Second Degree AV Block (Mobitz type I, Wenkebach
59 Rate P wave QRS variable normal morphology with constant P-P interval normal Conduction the P-R interval is progressively longer until one P wave is blocked; the cycle begins again following the blocked P wave. Rhythm irregular
60 Second degree AV block type I occurs in the AV node above the Bundle of His. It is often transient and may be due to acute inferior MI or digitalis toxicity. Treatment is usually not indicated as this rhythm usually produces no symptoms

61 Third Degree AV Block or Complete AV Block
62 Rate P wave QRS Conduction Rhythm atrial rate is usually normal; ventricular rate is usually less than 70/bpm. The atrial rate is always faster than the ventricular rate. normal with constant P-P intervals, but not "married" to the QRS complexes. may be normal or widened depending on where the escape pacemaker is located in the conduction system atrial and ventricular activities are unrelated due to the complete blocking of the atrial impulses to the ventricles. irregular
63 Complete block of the atrial impulses occurs at the A-V junction, common bundle or bilateral bundle branches. Another pacemaker distal to the block takes over in order to activate the ventricles or ventricular standstill will occur. May be caused by: digitalis toxicity acute infection MI and degeneration of the conductive tissue.
64 Treatment modalities include: external pacing and atropine for acute, symptomatic episodes and permanent pacing for chronic complete heart block

65 Bundle Branch Block
66 Rate P wave QRS variable normal if the underlying rhythm is sinus wide; > 0.12 seconds Conduction This block occurs in the right or left bundle branches or in both. The ventricle that is supplied by the blocked bundle is depolarized abnormally. Rhythm regular or irregular depending on the underlying rhythm
67 Left bundle branch block is more ominous than right bundle branch block because it usually is present in diseased hearts. Both may be caused by hypertension, MI, or cardiomyopathy. A bifasicular block may progress to third degree heart block. Treatment is artificial pacing for a bifasicular block that is associated with an acute MI.

68 Premature Ventricular Contractions
69 Rate P wave QRS Conduction Rhythm variable usually obscured by the QRS, PST or T wave of the PVC wide > 0.12 seconds; morphology is bizarre with the ST segment and the T wave opposite in polarity. May be multifocal and exhibit different morphologies. the impulse originates below the branching portion of the Bundle of His; full compensatory pause is characteristic. irregular. PVC's may occur in singles, couplets or triplets; or in bigeminy, trigeminy or quadrigeminy
70 PVCs can occur in healthy hearts. For example, an increase in circulating catecholamines can cause PVCs. They also occur in diseased hearts and from drug (such as digitalis) toxicities. Treatment is required if they are: associated with an acute MI, occur as couplets, bigeminy or trigeminy, are multifocal, or are frequent (>6/min).

71 Ventricular Tachycardia
72 Rate usually between 100 to 220/bpm, but can be as rapid as 250/bpm P wave QRS Conduction Rhythm obscured if present and are unrelated to the QRS complexes. wide and bizarre morphology as with PVCs three or more ventricular beats in a row; may be regular or irregular
73 Ventricular tachycardia almost always occurs in diseased hearts. Some common causes are: CAD acute MI digitalis toxicity CHF ventricular aneurysms. Patients are often symptomatic with this dysrhythmia
74 Ventricular tachycardia can quickly deteriorate into ventricular fibrillation. Electrical countershock is the intervention of choice if the patient is symptomatic and rapidly deteriorating. Some pharmacological interventions include lidocaine, pronestyl, and bretylium

75 Torsade de Pointes
76 Rate usually between 150 to 220/bpm, P wave obscured if present QRS wide and bizarre morphology Conduction Rhythm as with PVCs Irregular
77 Paroxysmal starting and stopping suddenly Hallmark of this rhythm is the upward and downward deflection of the QRS complexes around the baseline. The term Torsade de Pointes means "twisting about the points." Consider it V-tach if it doesn t respond to antiarrythmic therapy or treatments Caused by: drugs which lengthen the QT interval such as quinidine electrolyte imbalances, particularly hypokalemia myocardial ischemia
78 Treatment: Synchronized cardioversion is indicated when the patient is unstable. IV magnesium IV Potassium to correct an electrolyte imbalance Overdrive pacing
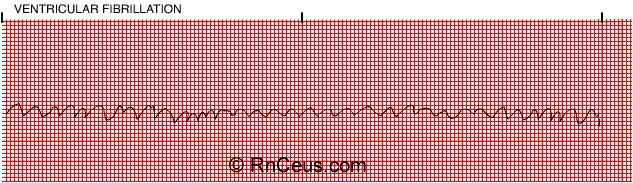
79 Ventricular Fibrillation
80 Rate P wave QRS Conduction unattainable may be present, but obscured by ventricular waves not apparent chaotic electrical activity Rhythm chaotic electrical activity
81 This dysrhythmia results in the absence of cardiac output. Almost always occurs with serious heart disease, especially acute MI. The course of treatment for ventricular fibrillation includes: immediate defibrillation and ACLS protocols. Identification and treatment of the underlying cause is also needed
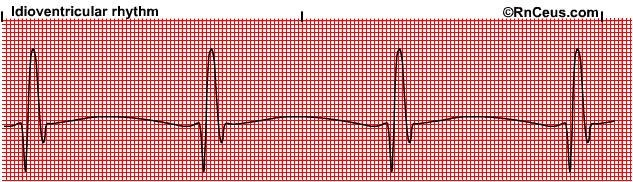
82 Idioventricular Rhythm
83 Rate 20 to 40 beats per minute P wave QRS Absent Widened Conduction Failure of primary pacemaker Rhythm Regular
84 Absent P wave Widened QRS > 0.12 sec. Also called " dying heart" rhythm Pacemaker will most likely be needed to re-establish a normal heart rate.
85 Causes: Myocardial Infarction Pacemaker Failure Metabolic imbalance Myoardial Ischemia Treatment goals include measures to improve cardiac output and establish a normal rhythm and rate. Options include: Atropine Pacing Caution: Supressing the ventricular rhythm is contraindicated because that rhythm protects the heart from complete standstill.
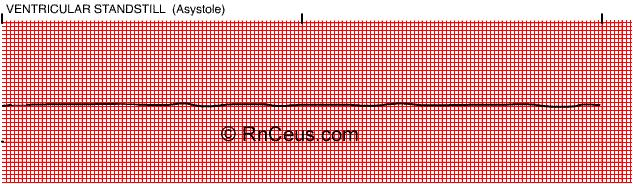
86 Asystole/Ventricular Standstill
87 Rate none P wave may be seen, but there is no ventricular response QRS Conduction Rhythm none none none
88 Asystole occurs most commonly following the termination of atrial, AV junctional or ventricular tachycardias. This pause is usually insignificant. Asystole of longer duration in the presence of acute MI and CAD is frequently fatal. Interventions include: CPR, artificial pacing, and atropine.
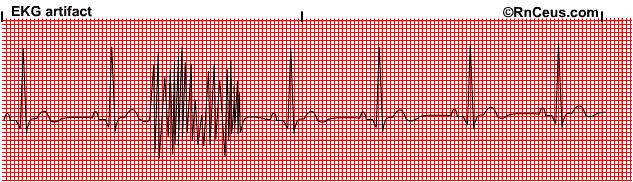
89 Artifact
90 Artifact occurs when something causes a disruption in monitoring. Some common causes are: AC interference -causes 60 cycle artifact Muscle tremors Respiratory artifact-wandering baseline Loose electrode Broken lead wire
91 WCT: Wide Complex Tachycardia How to differentiated between VT vs SVT, basic features Rate The rate of the WCT is of limited use in distinguishing VT from SVT Regularity - Slight irregularity suggests VT as opposed to most SVTs Axis - A right superior axis (axis from -90 to ±180º), sometimes called an indeterminate or "northwest" axis, is strongly suggests VT In a patient with a RBBB-like WCT, a QRS axis to the left of -30º suggests VT In a patient with an LBBB-like WCT, a QRS axis to the right of +90º suggests VT QRS duration >140 msec suggests VT; while in a LBBB-like WCT, a QRS duration >160 msec suggests VT Concordance is present when the QRS complexes in all six precordial leads (V1 through V6) are monophasic with the same polarity
92 AV Dissociation Dissociated P waves PP and RR intervals are different PR intervals are variable There is no association between P and QRS complexes The presence of a P wave with one, but not all, QRS complexes Fusion beats Capture beats
93 ALGORITHMS FOR WCT DIAGNOSIS
94 QRS morphology V1 positive (RBBB) pattern Findings in V1 A monophasic R or biphasic qr complex in V1 favors VT. A triphasic RSR' or RsR' complex (the so-called "rabbit-ear" sign) with left peak of the RsR' complex is taller than the right peak, VT is more likely Findings in lead V6 An rs complex (R wave smaller than S wave) in lead V6 favors VT. In contrast, an Rs complex (R wave larger than S wave) in lead V6 favors SVT.
95 V1 negative (LBBB) pattern Findings in lead V1 or V2 A broad initial R wave of 40 msec duration or longer in lead V1 or V2 favors VT Slurred or notched downstroke of the S wave in lead V1 or V2, Duration from the onset of the QRS complex to the nadir of the QS or S wave of 60 msec in lead V1 or V2. Findings in lead V6 The presence of any Q or QS wave in lead V6 favors VT
96 AVR Criteria
97 NCT: Narrow Complex Tachycardia Regularity Regular sinus tachycardia, A.flutter, AT, AVNRT, AVRT Irregular AF, MAT P wave Regular with P ST, AT, A.Flutter, AVRT, AVNRT Regular without P AVNRT Irregular with P MAT Irregular without P - AF
Basic Dysrhythmia Interpretation
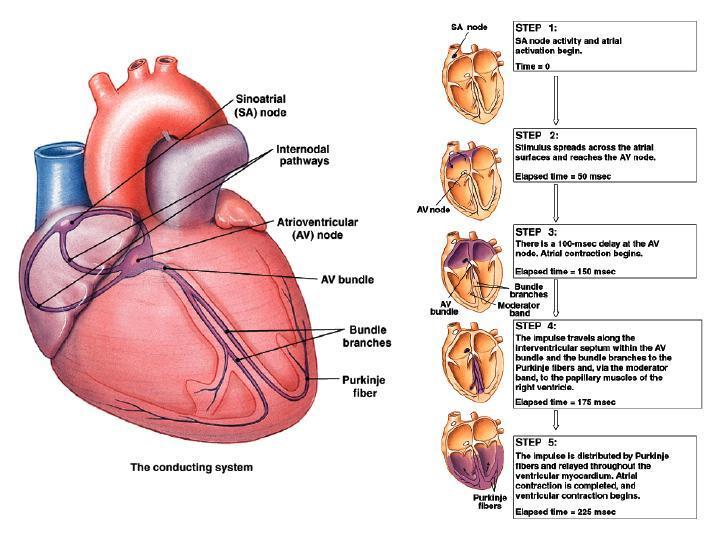
 Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Junctional Premature Contraction (JPC)
") Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT
 Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms
 Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Chapter 9: Ventricular Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 9.1 Describe the various ventricular dysrhythmias 9.2
Electrocardiography for Healthcare Professionals Chapter 9: Ventricular Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 9.1 Describe the various ventricular dysrhythmias 9.2
Cardiac Arrhythmias in Sleep
 Cardiac Arrhythmias in Sleep Only 53 Slides! Gauresh H Kashyap, MD, FACP, FCCP, FAASM 1 2 Cardiac Arrhythmias in Sleep Out of 400 Patients with OSA, 48% had some Arrhythmias 20% - 2 PVCs/min 7% - Bradycardia
Cardiac Arrhythmias in Sleep Only 53 Slides! Gauresh H Kashyap, MD, FACP, FCCP, FAASM 1 2 Cardiac Arrhythmias in Sleep Out of 400 Patients with OSA, 48% had some Arrhythmias 20% - 2 PVCs/min 7% - Bradycardia
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Rate: The atrial and ventricular rates are equal; heart rate is greater than 100 bpm (usually between bpm).
.") Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
HTEC 91. Performing ECGs: Procedure. Normal Sinus Rhythm (NSR) Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway
 Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway") HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Rhythm Interpretation Exam
 as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Basic EKG Interpretation. Nirja Parikh, PT, DPT
 Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
COURSE DESCRIPTION. Rev 2.0 7/2013. Page 1 of 26
 COURSE DESCRIPTION Ventricular dysrhythmias (arrhythmias) are unique and potentially dangerous cardiac rhythms. They are often associated with Code Blue calls, and life and death situations. The only two
COURSE DESCRIPTION Ventricular dysrhythmias (arrhythmias) are unique and potentially dangerous cardiac rhythms. They are often associated with Code Blue calls, and life and death situations. The only two
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
5AB Dysrhythmia Interpretation tation and Management Review Please complete and return by:
 1 5AB Dysrhythmia Interpretation tation and Management Review 2014 RN Please complete and return by: Overview 2 This review begins with a discussion of the physiology of cardiac conduction, and then covers
1 5AB Dysrhythmia Interpretation tation and Management Review 2014 RN Please complete and return by: Overview 2 This review begins with a discussion of the physiology of cardiac conduction, and then covers
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
ECG Interpretation and Clinical Significance
 Confirming Pages ECG Interpretation and Clinical Significance Chapter Outline 5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 5.9 5.10 Learning Outcomes Key Terms Introduction (p. 114) Identifying the Components of the
Confirming Pages ECG Interpretation and Clinical Significance Chapter Outline 5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 5.9 5.10 Learning Outcomes Key Terms Introduction (p. 114) Identifying the Components of the
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
physiology 6 Mohammed Jaafer Turquoise team
 15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
2017 BDKA Review. Regularity Rate P waves PRI QRS Interpretation. Regularity Rate P waves PRI QRS Interpretation 1/1/2017
 1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
Making Sense of Those Little Lines Advanced ECG Interpretation
 Making Sense of Those Little Lines Advanced ECG Interpretation Cara Solodky-Hardy, ND, ANP-BC, AACC MD24 House Call Cardiology My patients www.ecglibrary.com Image Sources The Alan E. Lindsay Ecg Learning
Making Sense of Those Little Lines Advanced ECG Interpretation Cara Solodky-Hardy, ND, ANP-BC, AACC MD24 House Call Cardiology My patients www.ecglibrary.com Image Sources The Alan E. Lindsay Ecg Learning
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2
Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2
8/20/2012. Learning Outcomes (Cont d)
") 1 2 3 4 Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2 Identify premature junctional complexes
1 2 3 4 Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2 Identify premature junctional complexes
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
ECG (MCQs) In the fundamental rules of the ECG all the following are right EXCEP:
 In the fundamental rules of the ECG all the following are right EXCEP:") ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
ECG (MCQs) 2010 1- In the fundamental rules of the ECG all the following are right EXCEP: a- It is a biphasic record of myocardial action potential fluctuations. b- Deflection record occurs only during
Lecture outline. Electrical properties of the heart. Automaticity. Excitability. Refractoriness. The ABCs of ECGs Back to Basics Part I
 Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 5: Rhythm Strip Interpretation and Sinus Rhythms Learning Outcomes 5.1 Explain the process of evaluating ECG tracings
Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 5: Rhythm Strip Interpretation and Sinus Rhythms Learning Outcomes 5.1 Explain the process of evaluating ECG tracings
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
The ECG Course. Boone County Fire Protection District EMS Education
 The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Lab Activity 24 EKG. Portland Community College BI 232
 Lab Activity 24 EKG Reference: Dubin, Dale. Rapid Interpretation of EKG s. 6 th edition. Tampa: Cover Publishing Company, 2000. Portland Community College BI 232 Graph Paper 1 second equals 25 little boxes
Lab Activity 24 EKG Reference: Dubin, Dale. Rapid Interpretation of EKG s. 6 th edition. Tampa: Cover Publishing Company, 2000. Portland Community College BI 232 Graph Paper 1 second equals 25 little boxes
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
ACLS Study Guide for Precourse Self-Assessment
 20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
Miscellaneous Stuff Keep reading the Outline
 Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C. For more presentations
 ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
ELECTROCARDIOGRAPHY KEVIN REBECK PA-C For more presentations www.medicalppt.blogspot.com Objectives ECG History Pathophysiology Basics Case Historys Electrical activation of the heart In the heart
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
PEDIATRIC EKG WORKSHOP
 WHAT s NEW IN MEDICINE 2018 PEDIATRIC EKG WORKSHOP Salaam Sallaam, MD Asst. Prof, Division of Cardiology Department of Pediatrics Seattle Children s Hospital OVERVIEW Pediatric EKG interpretation Normal
WHAT s NEW IN MEDICINE 2018 PEDIATRIC EKG WORKSHOP Salaam Sallaam, MD Asst. Prof, Division of Cardiology Department of Pediatrics Seattle Children s Hospital OVERVIEW Pediatric EKG interpretation Normal
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
INDEX. Kingston General Hospital May Introduction Page 2. Cardiac Conduction System Page 3. Introduction to Cardiac Monitoring Page 5
 Kingston General Hospital May 2008 INDEX Introduction Page 2 Cardiac Conduction System Page 3 Introduction to Cardiac Monitoring Page 5 Recording Electrical Events Page 9 Waves of the ECG Complex Page
Kingston General Hospital May 2008 INDEX Introduction Page 2 Cardiac Conduction System Page 3 Introduction to Cardiac Monitoring Page 5 Recording Electrical Events Page 9 Waves of the ECG Complex Page
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
ECGs on the acute admission ward. - Cardiology Update -
 ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
Cardiac Telemetry Self Study: Part One Cardiovascular Review 2017 THINGS TO REMEMBER
 Please review the above anatomy of the heart. THINGS TO REMEMBER There are 3 electrolytes that affect cardiac function o Sodium, Potassium, and Calcium When any of these electrolytes are out of the normal
Please review the above anatomy of the heart. THINGS TO REMEMBER There are 3 electrolytes that affect cardiac function o Sodium, Potassium, and Calcium When any of these electrolytes are out of the normal